




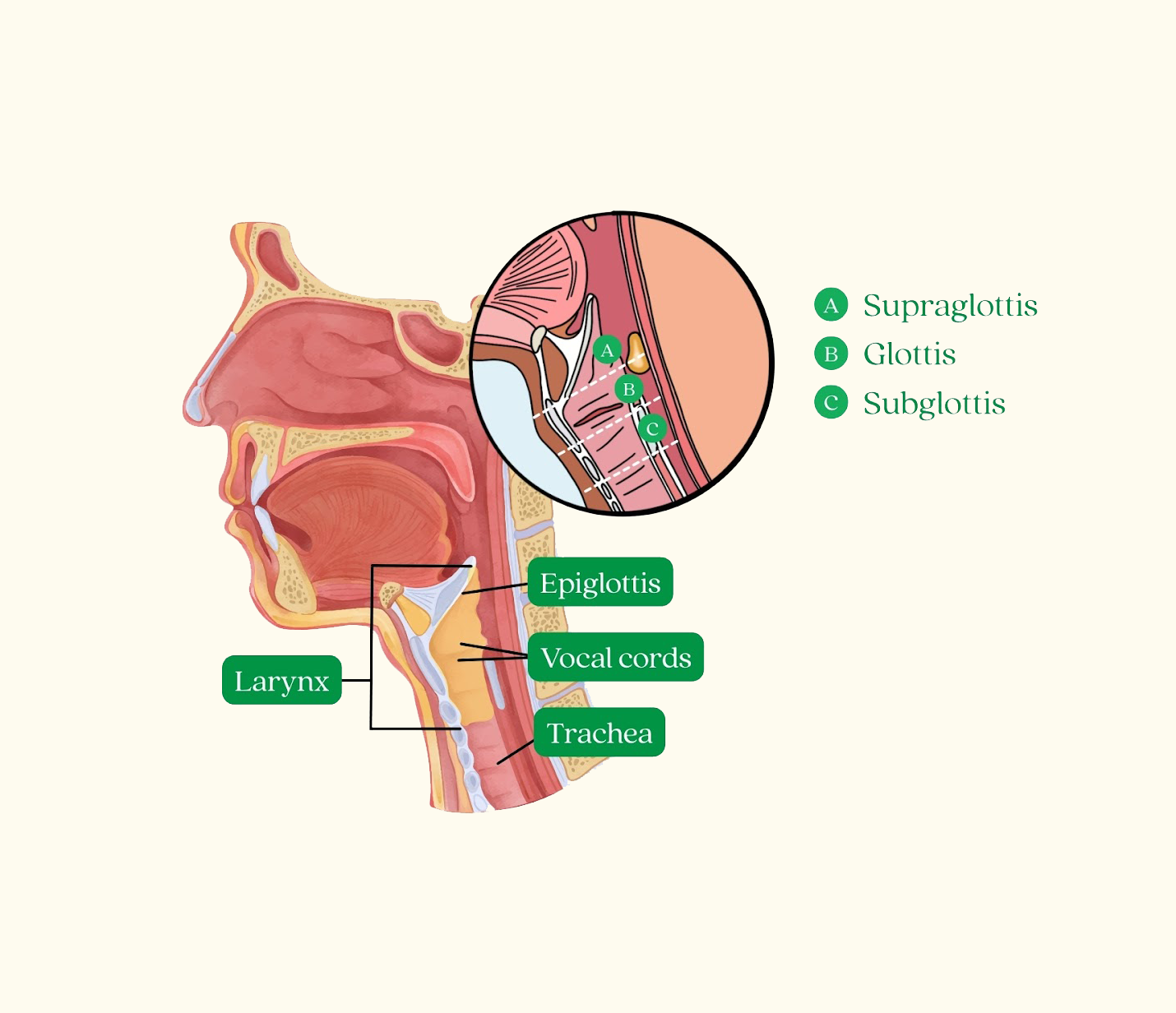
Laryngeal cancer is a cancer that develops in the larynx, commonly known as the voice box. The larynx sits in the throat between the pharynx and the trachea (windpipe). It plays an important role in breathing, speaking, and protecting the airway during swallowing.

Most cancers of the larynx are squamous cell carcinomas, arising from the lining of the laryngeal mucosa.
The larynx is divided into three main regions, and cancer can develop in any of these areas:
The location of the tumour can influence symptoms, staging, and treatment approach.
Laryngeal cancer is rare in Singapore and contributes a small share of all cancers.
It occurs more often in men and is usually diagnosed in adults older than 50 years.
Major risk factors include tobacco use and heavy alcohol consumption.
Common warning symptoms include persistent hoarseness and ongoing voice change.
Because symptoms may appear relatively early, some cases are identified at an earlier stage than other cancers of the head and neck.

Symptoms of laryngeal cancer depend on the location and size of the tumour within the voice box. In many cases, cancers affecting the vocal cords cause early voice changes, which may prompt earlier medical evaluation.
Common Symptoms
Other Symptoms That May Occur
These symptoms may occur particularly as the tumour grows or spreads to nearby structures.
Symptoms that persist for more than 2–3 weeks should be medically evaluated, especially persistent hoarseness without an obvious cause such as infection or voice strain.

The diagnosis of laryngeal cancer involves a combination of clinical examination, endoscopic evaluation, imaging studies, and tissue biopsy. A definitive diagnosis requires microscopic examination of tumour tissue.
In most cases, the initial evaluation is performed by an ear, nose and throat (ENT) specialist, and further management may involve a multidisciplinary team that includes medical oncologists, head and neck surgeons, and supportive and palliative care specialists.
The doctor will assess symptoms and potential risk factors, including:
A head and neck examination is performed, including assessment of the mouth, throat, and lymph nodes in the neck.
Laryngoscopy allows doctors to directly visualise the larynx and vocal cords.
A flexible laryngoscope, which is a thin camera inserted through the nose, is commonly used to examine the voice box. This procedure helps identify abnormalities such as:
In some cases, a more detailed examination under anaesthesia may be performed to allow better visualisation of the larynx.
If cancer is suspected or confirmed, imaging studies are performed to determine the size and extent of the tumour and whether it has spread to nearby structures or lymph nodes.
Common imaging tests include:
These imaging studies help guide staging and treatment planning.
A biopsy is required to confirm the diagnosis of laryngeal cancer.
During this procedure, a small tissue sample is taken from the suspicious area and examined under a microscope by a pathologist. Most laryngeal cancers are squamous cell carcinomas arising from the lining of the larynx.
Biopsy is often performed during direct laryngoscopy under general anaesthesia, which allows accurate sampling of the tumour.
Laryngeal cancer is staged using the TNM staging system developed by the American Joint Committee on Cancer (AJCC). The current system used in clinical practice is the AJCC 8th Edition.
Staging describes how far the cancer has spread and helps guide treatment planning.
The TNM system evaluates three key components:
Based on these findings, the disease is grouped into Stage I to Stage IV.
The tumour is small and confined to one part of the larynx.
The vocal cords may still move normally, and there is no spread to lymph nodes or distant organs.
The tumour has grown larger or involves more than one nearby area within the larynx but has not spread to lymph nodes or distant organs.
Voice changes or hoarseness may occur depending on the tumour location.
The tumour has grown further within the larynx and may affect vocal cord movement or nearby tissues.
Cancer may also have spread to a single lymph node in the neck on the same side.
Stage IV represents more advanced disease.
The tumour may have spread beyond the larynx into nearby structures such as the thyroid cartilage, surrounding soft tissues, or other parts of the neck.
Cancer may also involve multiple lymph nodes or spread to distant organs.
Stage IV is often further divided into IVA, IVB, and IVC, depending on the extent of local invasion, lymph node involvement, or distant metastasis.

Treatment of laryngeal (voice box) cancer is individualised and typically planned through a multidisciplinary discussion. The goals are to control the cancer while preserving, where possible, speech, swallowing, and airway function.
Treatment decisions depend on:
Early laryngeal cancers are often treated with single-modality therapy, with good potential for larynx preservation:
Common options include:
Both approaches are widely accepted; choice depends on tumour factors and functional considerations (voice outcomes, swallowing, and patient preference).


More advanced disease usually requires multi-modality treatment. Common strategies include:
A total laryngectomy may be recommended when the tumour is extensive, airway function is compromised, or when organ-preservation strategies are not suitable.
If the cancer returns after initial treatment, or spreads to distant organs, management may include:
Supportive care is a core part of treatment planning, especially because laryngeal cancer and its treatments can affect voice, swallowing, and nutrition. Patients may benefit from:



