




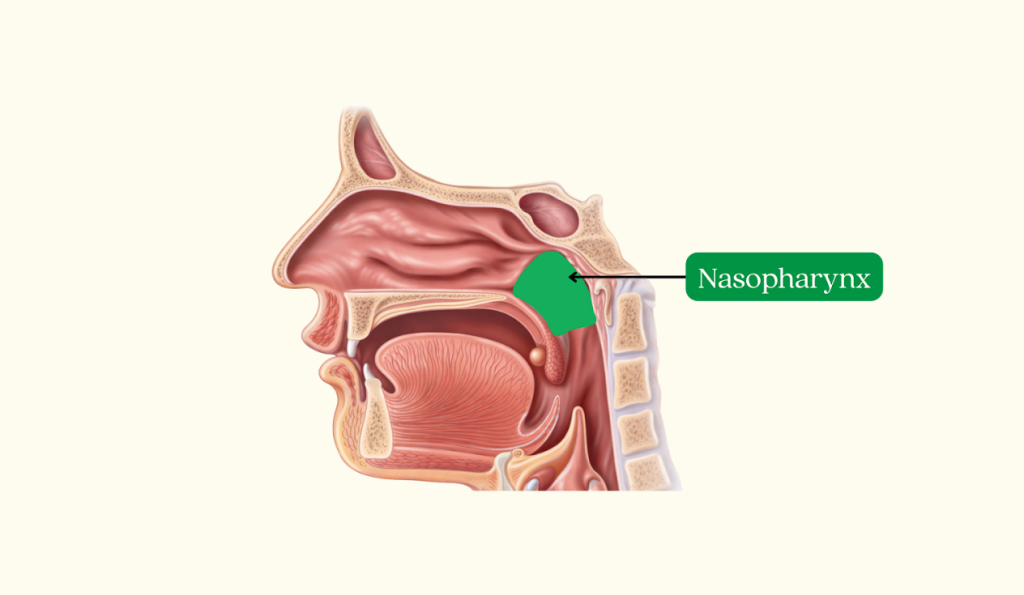
Nasopharyngeal cancer (NPC) is a cancer that starts in the nasopharynx, located behind the nose and above the back of the throat. It is a type of head and neck cancer. Because the nasopharynx sits behind the nose, some people mistakenly refer to it as “nose cancer,” although it is medically distinct.

Nasopharyngeal cancer is uncommon worldwide but has a significantly higher incidence in parts of East and Southeast Asia.
According to International Agency for Research on Cancer GLOBOCAN 2020 data:
Although incidence has gradually declined over the past decades, nasopharyngeal cancer remains one of the more distinctive cancers in Asian populations compared with Western countries, where it is rare.
Nasopharyngeal cancer may cause no symptoms at first, or only mild symptoms. When symptoms occur, they commonly involve the neck, nose, and ears because the nasopharynx sits behind the nose and near the Eustachian tube opening.
A painless lump in the neck due to enlarged lymph nodes is one of the most common presentations.
The diagnosis of nasopharyngeal cancer involves a combination of clinical examination, endoscopic evaluation, biopsy, and imaging tests. These investigations confirm the presence of cancer and determine the extent of disease.
Doctors begin with a detailed medical history and physical examination. The head and neck are examined carefully, including checking for enlarged lymph nodes in the neck.
A nasal endoscopy (also called nasoendoscopy) allows doctors to directly examine the nasopharynx using a thin, flexible camera inserted through the nose. This helps identify abnormal areas or growths at the back of the nose.
A biopsy is required to confirm the diagnosis. During this procedure, a small tissue sample from the suspicious area is taken and examined under a microscope to determine whether cancer cells are present. Nasoendoscopy together with biopsy remains the gold standard for confirming nasopharyngeal cancer.
Imaging studies are performed to determine the location and extent of the tumour and whether the cancer has spread to nearby structures or lymph nodes. These may include:
MRI is commonly used to assess the local extent of disease and involvement of surrounding structures.
Blood tests may be performed to detect markers related to Epstein-Barr virus infection, which is closely associated with nasopharyngeal cancer. Plasma Epstein Barr virus DNA may also be used in clinical assessment and monitoring.
After the diagnosis is confirmed, further tests are performed to determine the stage of the cancer. Staging helps doctors plan the most appropriate treatment.

Staging describes how far the cancer has spread in the body. For nasopharyngeal cancer, staging helps doctors determine the extent of the tumour and guides treatment planning.
Nasopharyngeal cancer is commonly staged using the TNM staging system, which evaluates:
Based on these findings, the disease is grouped into Stage I to Stage IV.
The cancer is confined to the nasopharynx and has not spread to lymph nodes or distant organs.
The tumour may have extended slightly beyond the nasopharynx or spread to nearby lymph nodes in the neck, but it has not spread to distant parts of the body.
The tumour may involve nearby bones, sinuses, or surrounding structures. Lymph node involvement in the neck may also be present.
This stage represents more advanced disease. The tumour may have spread to nearby critical structures such as the skull base or cranial nerves, involve more extensive lymph nodes, or spread to distant organs such as the lungs, liver, or bones.
Why Staging Matters
Staging helps doctors determine the most appropriate treatment approach and provides information about prognosis.
Treatment for nasopharyngeal cancer depends on the stage of the cancer, the extent of lymph node involvement, whether there is spread to other organs, and the patient’s overall health.



